Usually, I trace buildings and roads I can see on satellite imagery via the HOT Tasking Manager (HOT Tasking Manager). This morning, however, I grab a tea and sit down at my computer to dial into a meeting with my Médecins Sans Frontières (MSF) colleagues halfway across the world in Kulob, Tajikistan.
I share my screen with a satellite image of the city, and we get to work. Today, we are working together to draw the boundaries of the city’s neighbourhoods. Pouring over the shared screen, the team in Kulob tell me where the boundary is. I draw it on my computer. As we go, we use railway stations, oddly shaped buildings, and marketplaces to find our way around the image and define the extent of neighbourhoods that are not available on any public map.
Together, we are creating new map data to use in the analysis a Tuberculosis project in this Central Asian country.
Tuberculosis in Tajikistan
Tuberculosis (TB) is an infectious disease caused by bacteria that most often affects the lungs. Tajikistan faces a high TB burden and the Kulob City of the Khatlon Region in southern Tajikistan with the four surrounding Jamoats (sub-districts), have one of the highest numbers of TB rates in the country. MSF initiated Zero TB project to demonstrate the feasibility of TB elimination, of which active case finding is a part. This public health strategy serves to proactively identify individuals with active TB disease who have not sought care themselves.
Fig x The map highlights the Kulob District in the southwest of Tajikistan.
The active case finding used computer-aided detection coupled with chest radiography (CAD4TB) at different sites. This is a mobile, digital X-ray system that can analyse a chest X-ray in less than a minute and can help identify individuals who need to go to a health centre for confirmatory testing.
 Kamola Rasulova/MSF") Fig x An MSF nurse is registering a villager who came for screening to a temporary X-ray facility set up by the project staff in Zarbdor village, Kulob, Tajikistan. (c) Kamola Rasulova/MSF
Fig x An MSF nurse is registering a villager who came for screening to a temporary X-ray facility set up by the project staff in Zarbdor village, Kulob, Tajikistan. (c) Kamola Rasulova/MSF
From the beginning of the project, mapping diagnosed TB patients was seen as an important part to inform screening, prevention, and educational activities to curtail transmission.
Understanding patient origins
The big questions that the Missing Maps team in MSF was invited to help with addressed the patient origins. Where did the patients come from? Where should the screening of the population take place? To answer these, we needed better map data.
Health Catchment Areas are geographic regions that a health facility will draw its patients from. Within the Kulob City neighbourhoods often act as a Health Catchment Area. A local neighbourhood might consist of a few streets that share a name, but there was no existing map of these geographic areas. To use the existing medical data to help focus activities, we needed to know where the neighbourhoods were. This would permit us to calculate the cases of TB per population and therefore, identify any TB hotspots.
Drawing on many sources
This research project tapped into a rich network of expertise and experience, and a wide set of tools. It was a collaboration between the public health specialist, the GIS team, epidemiologists and TB advisors from MSF UK, and the MSF health team in Kulob, Tajikistan.
We ran a remote mapping campaign of the Kulob district on the HOT Tasking Manager. We invited the Missing Maps volunteers to map residential areas, roads, and waterways on OpenStreetMap (OSM). Digitising satellite imagery provided a great launchpad for further refining our maps.
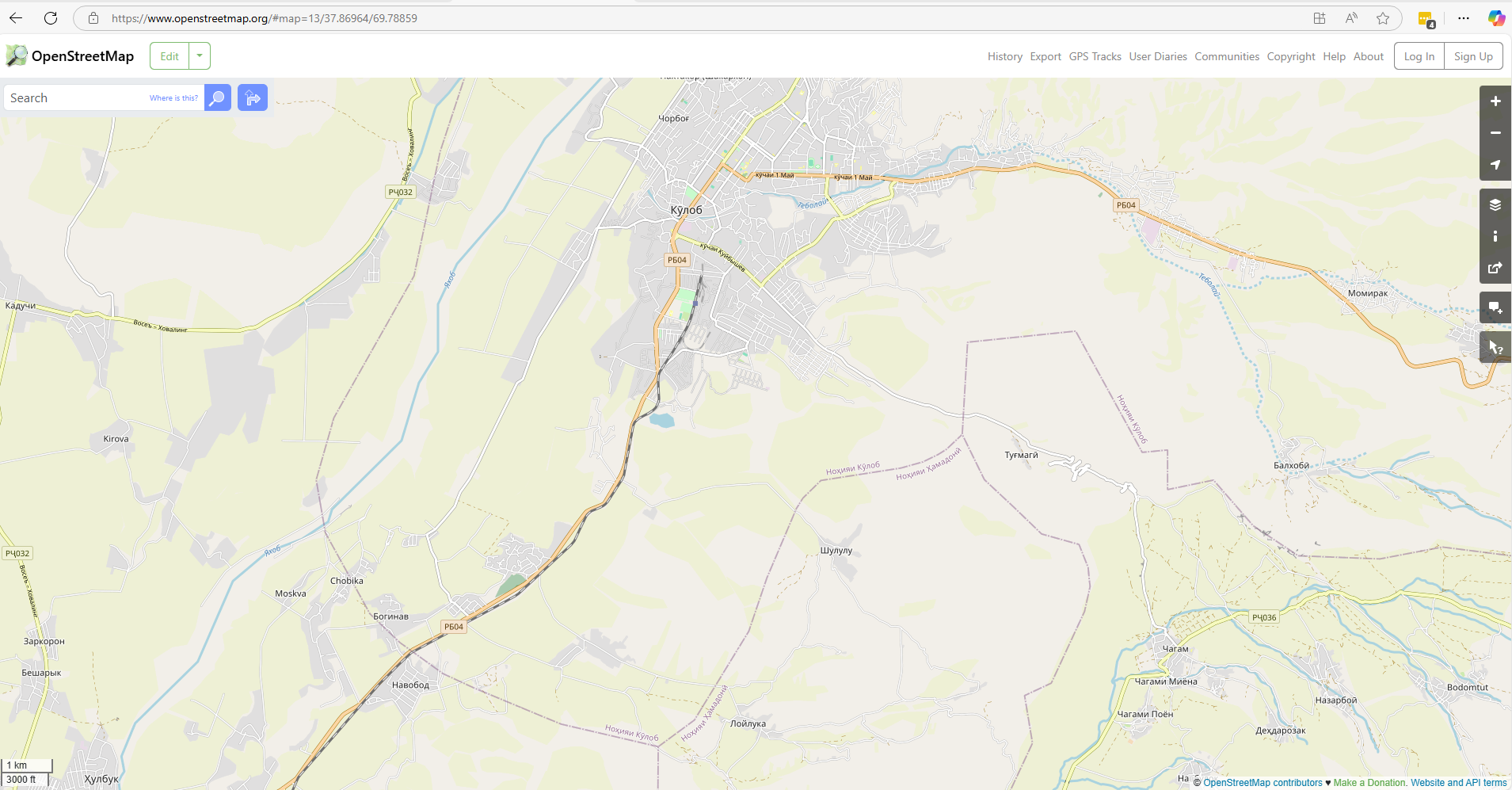
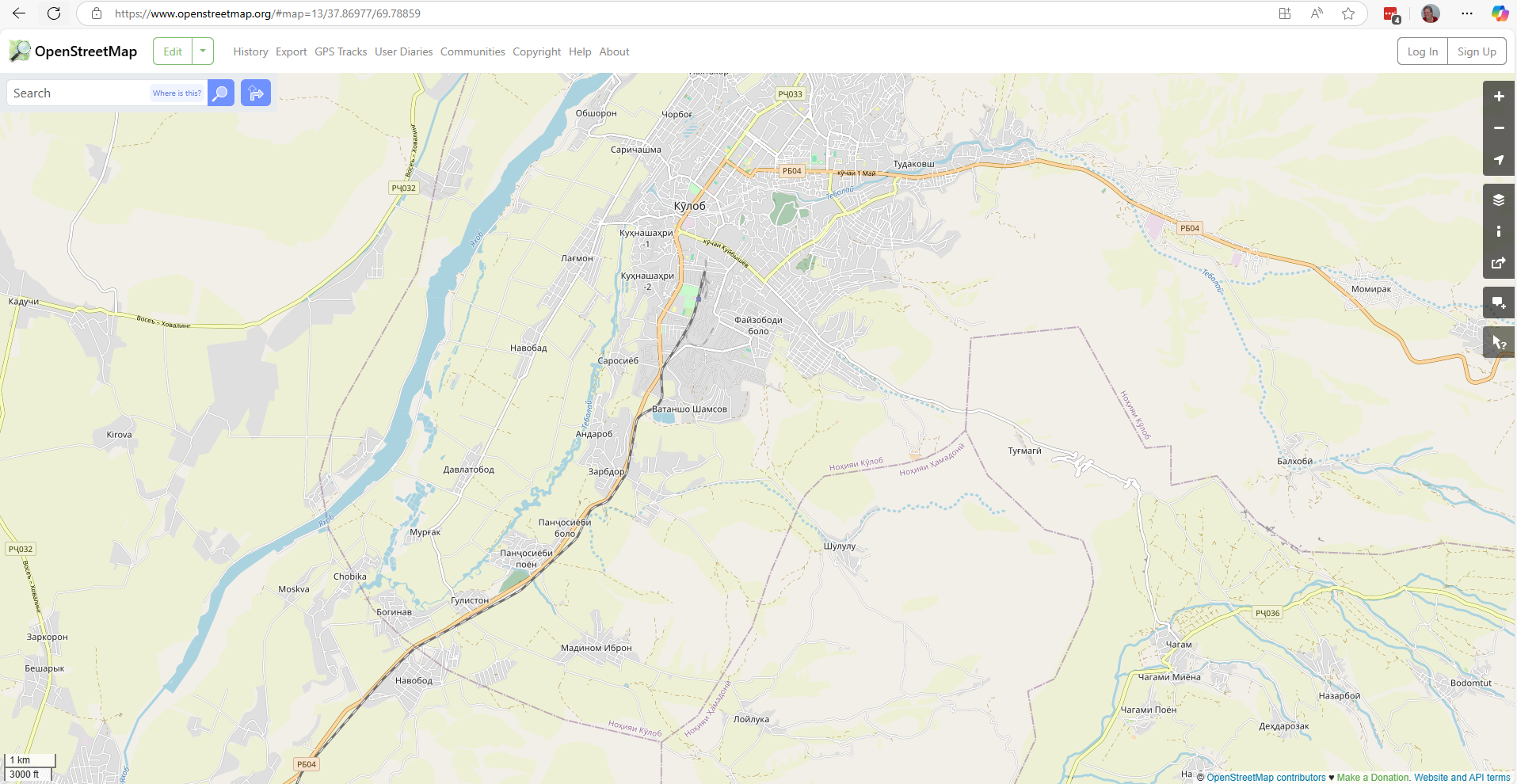 Both and after screenshots that show new data on OSM @OpensStreetMap contributors
Both and after screenshots that show new data on OSM @OpensStreetMap contributors
Subsequently, the team in Kulob used Field Papers to draw the outlines of neighbourhoods in the city. It is a tool for easily creating a printable map of OSM data that permits sketching onto it. The hand-drawn paper maps were photographed and sent back to me for digitisation.
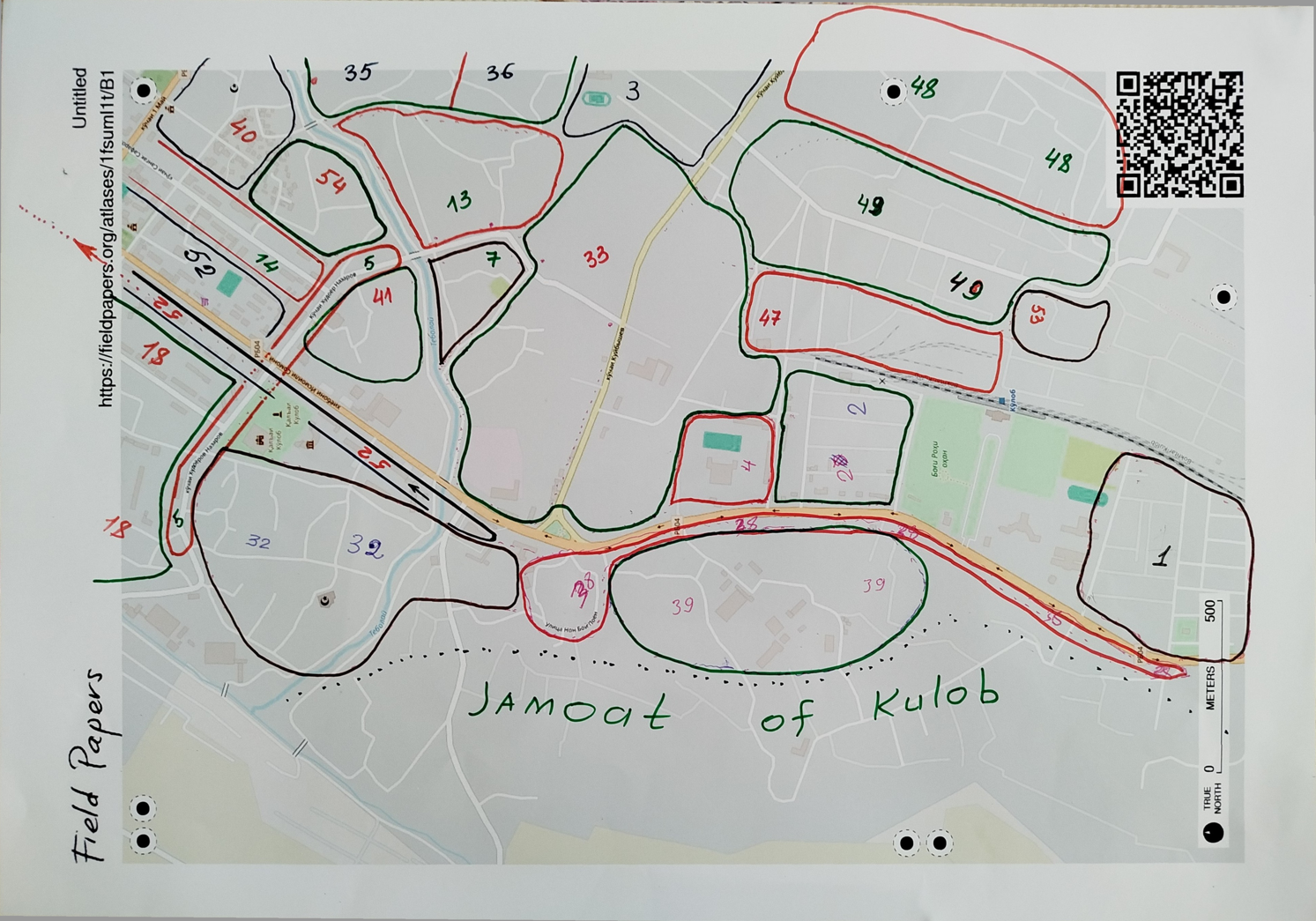 Fig x One page of the finished Field Papers that highlights the approximate boundaries of Kulob City neighbourhoods.
Fig x One page of the finished Field Papers that highlights the approximate boundaries of Kulob City neighbourhoods.
During follow-up visits to TB patients, MSF health teams collected GPS locations at their homes, as well as their addresses. This was another important source of information for our work to understand which streets and houses belong to which neighbourhood. These are the sorts of things that are unclear from a satellite image and impossible to determine without local knowledge.
The main component of a Kulob City address is the neighbourhood, and this was a crucial piece of information we were missing.
Local knowledge
On the other side of the screen, the team in Kulob consists of health promoters, drivers, and translators to facilitate the communication between English and Tajik. The health promotion officers and drivers have encyclopaedic knowledge of the neighbourhoods, so they are the right people to help me finetune the emerging map.
Slowly, our map takes form, as we shift the boundary to include or exclude specific roads and buildings. Also, we check the latest names for each neighbourhood. Some tricky bits cause a prolonged discussion between the drivers, sometimes only solved through a call to someone else to confirm a boundary.
By the end of an hour and a half, my cold cup of tea sits next to me, and we are ready to stop for the day. This joint work requires a lot of concentration, and we space the calls over several weeks. Over the course of the calls, the team members share little titbits of information about the buildings we see, correct my attempts at pronouncing place names in Tajik, and offer to take me to the striking amphitheatre we can see on the satellite imagery, should I ever find myself in Kulob.
 Fig x Maria digitising the field papers from Kulob, Tajikistan.
Fig x Maria digitising the field papers from Kulob, Tajikistan.
The result of this process is a map of the neighbourhoods of Kulob city and the outlying districts ready for the analysis of the spread of TB cases. This will also be a useful map for the local health promotion teams as they do their regular work.
Using the map
As fun and important as is it to create updated maps, the spatial analysis was an important part of the project as well. The research project retrospectively analysed medical data collected between January 2022 and December 2024. The geolocation data was integrated with population data to help identify TB transmission hotspots and calculate case notification rates. Further analysis by epidemiologists and TB experts was presented alongside our maps at the Regional Workshop on WHO Guidelines which was a capacity-building workshop in Kazakhstan in 2025 for twelve TB high-priority countries of the WHO European Region.
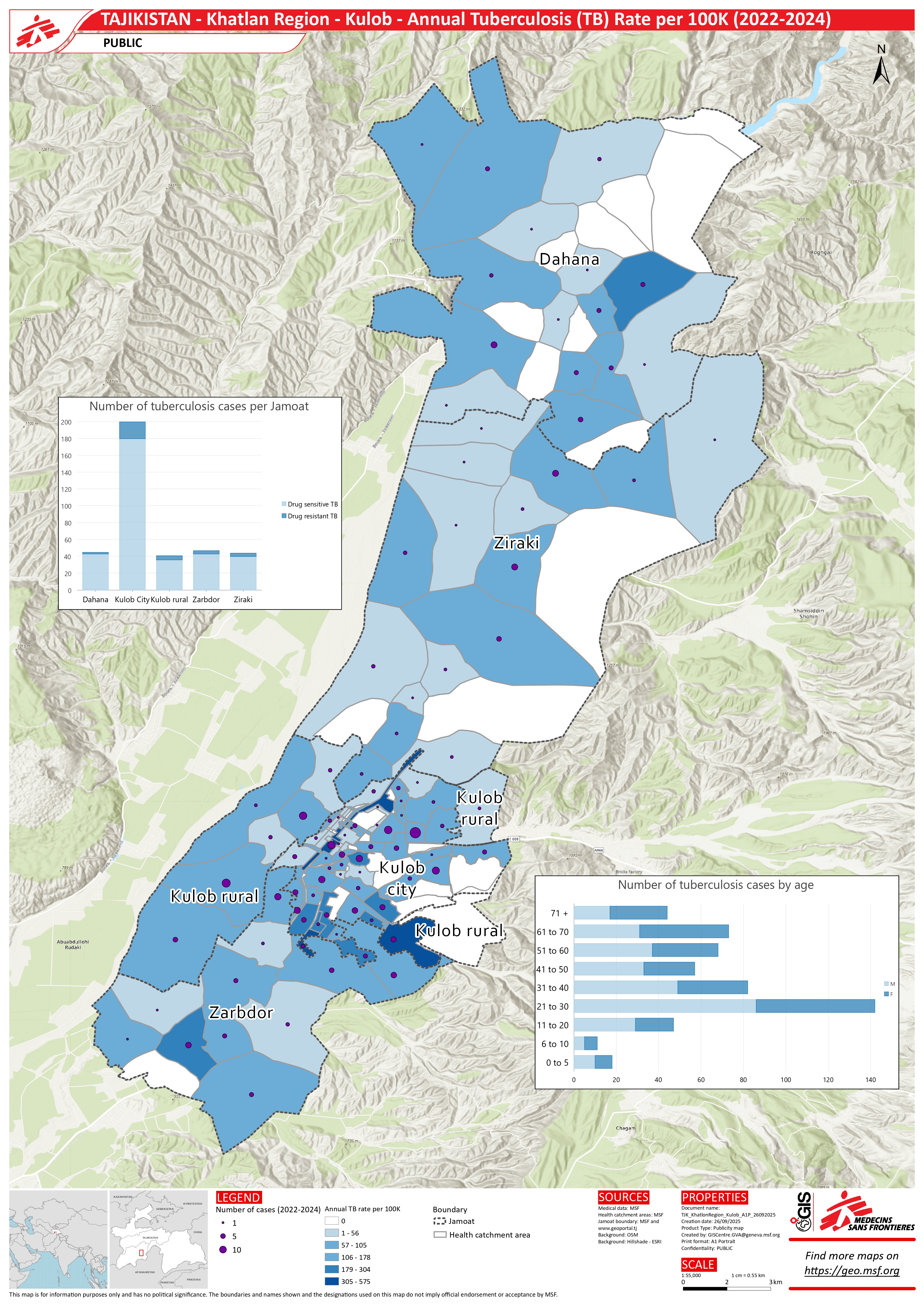 Fig 3. A map showing the annual rate of TB per 100,000 people.
Fig 3. A map showing the annual rate of TB per 100,000 people.
The names of neighbourhoods and street were shared on OpenStreetMap, ready and available for whoever needs it next. See for yourself what this looks like in Kulob. This close collaboration combined local knowledge with remote mapping, enabling accurate patient origin mapping and opportunities for targeted screening planning.
Moving from remote base-mapping to integrating local knowledge
This project gave me a fascinating opportunity to map intangible boundaries in a collaborative way and experience enriching the map with local knowledge first-hand. OSM data created through Missing Maps is a springboard for so much more, as this research project example shows. What is more, it can be a blueprint for similar mapping support for an epidemiological analysis, including in Kyrgyzstan and Uzbekistan, where MSF has also had TB-related projects.
I’m very grateful to the huge pool of people who provided their time, knowledge, and mentoring during this part of the research project and as we carry on taking steps to eliminate TB, including using GIS data.
As the Health Promotion Officer Askar Usmonov says, “The result of this project is that we now have a map that has been very useful for the project, especially mapping in the four jamoats. Other stakeholders can also use it. Due to this mapping we discovered new areas and new street names that we didn’t know about before”.
This project (and blog) would not have been possible without the support of Jose Luis Alvarez Moran, Animesh Sinha, Matthew Saunders, Jorieke Vyncke, Nash Naufal, Anna Farrow, Narmin Ali, Emmanuel Masumbuko, Norman Sitali, Askar Usmonov, Murod Abilov, Bibikhon Kandieva and Rahimjon Saydaliev.